This post was written in October 2019 but stayed on my phone until this week.
Hi, It’s the middle of the night. The hours of night are by far the loneliest, scariest and longest of complex care parenting. Fact.
This is even more true in hospital. If your child is going to do something unexpected and scary you can guarantee that it will be at night, and at the weekend. I’m pretty sure they get bonus points for the Friday night of a bank holiday weekend too.
We have been exceptionally lucky for the past few years that we have not needed to have any hospital stays but today we find ourselves six days into a post-operative stint in HDU and I’m finding that all the idiosyncrasies of life as an inpatient family as the same as they ever have been.
Truth One:
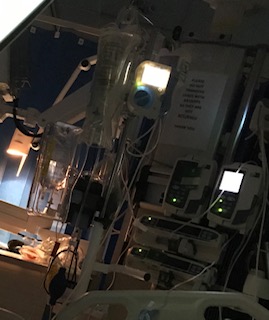
The beeping will drive you to the very edge of your last nerve. Don’t get me wrong I understand the importance of knowing what is going on with each little heartbeat, respiratory rate and oxygen saturation but unsurprisingly when children are in critical care, these numbers often are not what they should be and when that happens the machine beeps. And beeps. And beeps. Then the feeding pump beeps and the IV beeps and the medicine infusions beep and even the bloody bed itself beeps. It just doesn’t stop. Then on every ward there are 4 patients so multiply those beeps by 4 and you have the soundtrack to the HDU. On the plus side you can swear about it all you want as nobody will hear you over all the beeping.
Truth Two:
There is an insanely frustrating dichotomy between the intensity of the care required and the need for restorative sleep. To take our current stay as an example. Mojo has two nurses who take four observations every hour (blood pressure, temperature, pupil dilation and respiratory rate) on top of that she has her medication schedule which currently includes her 11 standard medication doses then morphine, diazepam, paracetamol and ibuprofen for pain. These are brought in every hour or so throughout the day. Then there is feeding, bed baths, two hourly repositioning to avoid pressure sores from her body cast. all of these things mean we see a nurse at least once every 30 minutes. This is before we start to count the medical teams involved. We are under HDU, Endocrine, Orthopaedic and Pain teams. They all do rounds independently so that is a minimum of 4 visits a day, all with physical examinations and some with blood testing. Then there are the therapy teams Occupational Therapy and Physio who need to move, manipulate and contort her. Finally the admin, cleaning, supplies, pharmacy, porters and catering teams who all pop in and out during the day (and night).
Don’t get me wrong, I completely understand how vital all these people are and how hard they are working to keep her well and safe but the end result is an utterly exhausted Mojo who drifts to sleep every twenty minutes only to be woken suddenly, in panic mode, thinking someone is about to do something that is going to hurt.
Truth Three:
This one is more true of HDU than of any other ward we’ve stayed on. In hospital you find some of life’s most extraordinary people. You will find them in the beds around you. Children going through some horrible, painful, unrelenting things and raising a smile through it all. Families walking through some of the worst days of their lives in a confined rectangle of space right next to other families doing the same.
It’s a weird kind of unspoken club, an atmosphere of sympathy, of empathy, of support, even when all that support can be is a knowing look or a consolatory smile.
The stories you hear on the ward, in the kitchen while you make tea or in a family room where people make calls updating family members, will break your heart. Utterly break it. It is when we stay in hospital that I understand why so many people say to us ‘I don’t know how you do it’ because I have that feeling of bewildered awe at the strength mustered by so many people to support their seriously ill child. We have done eight days and nights of this and we are on our knees with exhaustion, barely holding things together at home for the other kids. Many of these families have this as part of their everyday life. How do they do it I ask myself, the answer, of course is that you just do, you get out of your fold up bed, you have a strip wash over a sink and you get on with it.
Truth Four:
This is exactly the same but different. In hospital you find some of life’s most extraordinary people. This time, however, I mean on the other side of the story. The surgeons who do a job of such skill and responsibility that it makes me feel a bit sick just thinking about it. The doctors who deliver extraordinary bespoke care to each child despite unspeakable workloads, the nurses who care so sincerely and diligently, the therapists who shower praise for each micro-milestone. the guy who takes the food orders and behaves like he couldn’t be happier to see each and every child. The entertainer who visits each bed to sing songs and make balloon animals to distract from the pain for a while. The therapy dog (and his handler) who visits bedsides and shows off his frankly very impressive doggy Makaton. The guy who gets up, puts his Darth Vader costume on and comes to the Children’s Hospital to deliver some much needed escapism, after all a child that can defeat Darth Vader in a lightsabre battle can beat whatever else life throws at them, right? It never fails to astound me how hard people work in caring professions. The fact that people choose to dedicate their lives to improving the lives of others in such fundamental and extraordinary ways is something I will always feel grateful for.
Truth Five:
No matter how experienced you think you are and how able to cope with the emotional demands of life with a medically complex child there will be moments of absolute terror which take you by surprise. For me, ours came this evening when, after a reasonably stable post-op period she suddenly had a ‘funny turn’. Her heart rate skyrocketed and from nowhere her breathing was laboured and she was looking at me with fear in her eyes. Multiple people appeared by her bed. Lights went on. People were paged. I went from settling myself down to sleep to all consuming terror in seconds. In those few moments you fight the inner voices. The ones that say helpful things like ‘Oh God, this is it, she’s going to go, I’m losing her’. The voices which can be silenced during the day with reason, logic or even plain old denial are so loud and unwieldy at night. The smash you in the face awfulness of the term ‘Life Limiting Condition’, which you allow yourself to manage with the reassuring normality (our normal!) of day to day life, can knock the breath out of you at any point and every time is as terrifying as the first time. The she stabilises, medics start to look less panicked, everything calms down and your brain swiftly rebuilds its emotional self-defence mechanisms and you might have a little cry, dust yourself off and return to your fold out bed and plastic pillow.
Or you might lie awake writing about life in the HDU. That’s an option too.